Overview
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes.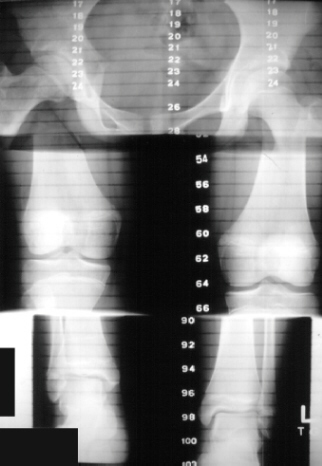
Causes
There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.

how we can increase our height?
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes.
Causes
There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.
how we can increase our height?
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
